
The COVID-19 virus has caused enormous worldwide disruption over the past several months. Just as this tiny virus has caused huge impacts, small changes in documentation have caused significant losses of vitally important revenue to our healthcare systems. Recently we have begun to see an increase in denials for COVID-19 diagnoses. With uncertainty regarding fiscal year reimbursements, elective surgeries volumes, and staffing, it is more important than ever for hospitals to get reimbursed at the appropriate level for the care of very sick patients, including patients with COVID-19.
Of course, first and foremost, we want to provide the interventions and treatment needed to restore our patients’ health and protect our communities. But, we also need to take care of the financial health of our hospitals. Complete, specific, and proper documentation will not only help the healthcare system’s revenue cycle, but it will also prevent retrospective audits and improve quality metrics for individual clinicians. How do we address this challenge? We must provide a higher level of specificity and clarity for cases where multiple conditions are contributing to making a patient very sick. The health of our hospitals depends upon us making this effort.
Documentation Tips for COVID-19
Coding for Risk Adjustment:
- Diagnose/document using coding-based language as much as possible
- Make sure the diagnosis(s) is in the chart at least once
- Document to the greatest level of specificity.
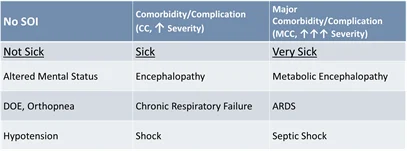
- Secondary Diagnoses: bucket into one of 3 groups – Not sick, sick, and very sick.
CDI Tips for COVID-19
Be specific with the following:
- Pneumonia – type, viral, bacterial (Gram Neg, MRSA, etc.), aspiration?
- Respiratory Failure – Acute, Chronic, Acute on Chronic?
- Sepsis – Septic shock, underlying infection, organism?
- Renal Failure – AKI, ATN, CKD, and stage?
- Type 2 MI – Demand Ischemia, underlying cause?
The New COVID-19 ICD-10-CM Code
- Applies to all patient types.
- The intent is to code for only confirmed cases of COVID-19.
- Provider’s diagnostic statement or a positive COVID-19 test result, assign code U07.1.
- The link between a positive test result and acute respiratory condition is not required.
- If COVID-19 test results are positive after discharge, Code U07.1 may be used.
- Assigning U07.1 as the principal diagnosis depends on the circumstances of admission.
It’s essential to keep in mind that the principal or secondary diagnosis of COVID-19 is based on the physician’s clinical judgment of how sick the patient is, notwithstanding a positive or negative test. Please remember that specificity is critical, not only for COVID-19 but for all documentation in the chart so that appropriate diagnoses, DRGs, and quality metrics to be assigned. Changing a few words can have an enormous impact on accurately portraying the severity of illness and the associated medical necessity issues.
Amid all of the confusion and uncertainty this pandemic has caused, this steadfast principle remains clear: the only defense against inappropriate COVID-19 denials is complete, specific, and appropriate documentation. Providers who paint a picture with their words significantly reduce the risk of being denied full reimbursement for treating these incredibly sick patients.
Dr. Wagstaff presented on this topic in the Sound Advisory Services webinar, COVID-19 Admissions: Getting Status Right & Preventing Denials. Click here to watch the webinar.
Sound Physician Advisory Services has a weekly newsletter, The Physician Advisor, where experts have curated relevant news articles, resources, and tools, along with breaking news on the pandemic into one newsletter. Click here to subscribe.